Gastrointestinal motility is one of the key factors determining the health of your intestinal flora. Before we get deeper into this section, I want to touch on a few important points regarding GI motility.
Methane and constipation
Constipation is often, but not always, linked to an overgrowth of methane-producing bacteria in the intestinal track. Studies have shown methane slows intestinal motility. In one study, researchers injected methane into the digestive track of dogs, which promptly reduced intestinal motility by 59%. 2014 review of the role of methane and intestinal motility says the following:
Table 3 summarizes seven adult studies that included 171 and 287 methane producers and non-producers, respectively. There is a clear association of methane production and slow intestinal transit, irrespective of health status (healthy, IBS or constipated individuals).
Triantafyllou, K., Chang, C. & Pimentel, M. Methanogens, methane and gastrointestinal motility. J Neurogastroenterol Motil 20, 31–40 (2014). https://www.ncbi.nlm.nih.gov/pubmed/24466443
Other studies have provided evidence that eliminating excess methane production in the intestines normalizes motility and reduces gastrointestinal symptoms (bloating, gas, abdominal pain, etc.). This matches my experience. After going through this program, eating onions and other high FODMAP foods no longer causes constipation; now eating those foods tends to give me loose stools.
The larger point is that correcting constipation by showing down fiber and laxatives isn’t helpful. They may increase motility but won’t fix the underlying problem of excess methane production. Antimicrobial herbals and diet that restricts fermentable carbohydrates should drastically reduce methane-producing bacteria in the gut. In most cases this gets rid of constipation and normalizes bowel movements.
Migrating motor complex (MMC)
Just like your kitchen needs regular cleaning and sweeping not to be infested with bugs, so do your intestines. The muscles in the small intestine go through periodic contraction and relaxation that produce a wave-like motion that pushes undigested food, bacteria, and other debris through the small intestine and into the large intestine. These peristaltic waves are called the migrating motor complex (MMC).
MMC is thought to be responsible for ‘house cleaning’ in the small intestine. Wikipedia on migrating motor complex:
The MMC occurs every 90-120 minutes during the interdigestive phase (between meals), and is responsible for the rumbling experienced when hungry. It also serves to transport bacteria from the small intestine to the large intestine, and to inhibit the migration of colonic bacteria into the terminal ileum.
There’s good evidence to show hindered MMC is at least partially responsible for SIBO. For examples, SIBO frequently occurs when MMC is suppressed with drugs. This makes sense given that the purpose of the MMC is to clear the small intestine from food and bacteria as well as prevent bacteria from migrating up from the large intestine.
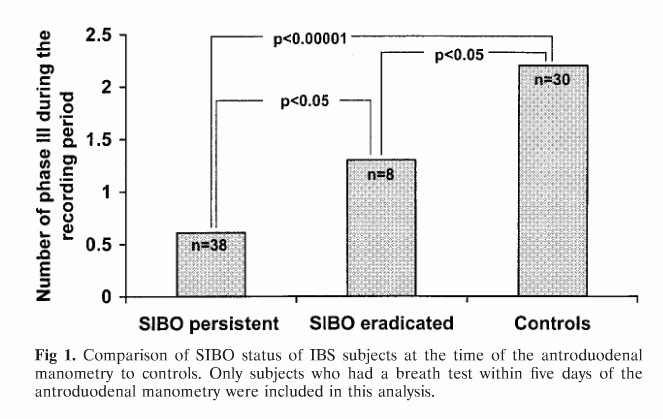
A 2002 study compared MMC function between people with SIBO and healthy controls. This graph shows the results for before and antibiotic treatment for SIBO patients and healthy controls.
Source: Pimentel, M., Soffer, E. E., Chow, E. J., Kong, Y. & Lin, H. C. Lower frequency of MMC is found in IBS subjects with abnormal lactulose breath test, suggesting bacterial overgrowth. Dig. Dis. Sci. 47,2639–43 (2002). https://www.ncbi.nlm.nih.gov/pubmed/12498278
The researchers conclude:
In conclusion, this study has found that a subgroup of IBS subjects with SIBO seem to have altered interdigestive motility. Infrequent and short-duration phase III seems to be characteristic of these subjects. Since phase III is important in cleansing the small intestine between meals, this finding may explain the SIBO.
The phase III they refer to is one of the four phases of the MMC.
The takeaway from this study is that the MMC is weak in people with SIBO. Eradicating SIBO with antibiotics to some degree restores MMC, but even after SIBO is eradicated the MMC remains much weaker than in healthy people. This, at least partially, explains why SIBO often recurs.
Dr. Allison Siebecker in her article about SIBO says that not using prokinetics (support motility) is one of the reasons patients don’t get better.
Fasted vs. fed sate
It’s important to note that MMC only occurs when you are in a ‘fasted’ state; meaning a few hours after a meal. Eating something puts you back into a ‘fed’ state and stops the MMC.
Most of this intestinal cleaning happens during the night. So it’s important to:
- not to eat large meals in the evening, and
- eat as little as possible (preferably nothing) for 2 to 3 hours before going to bed.
This ensures you are going to be in a fasted state and your intestines have enough time to clean up.
Stress
There’s some evidence to suggest stress reduces MMC and thus increases the risk of SIBO.
Don’t smoke weed
For centuries, Cannabis has been used to treat diarrhea. While there aren’t many human studies, there are plenty of animal studies that show cannabis slows motility throughout the entire digestive track.
Critically, it has been shown to reduce motility and MMC in the small intestine:
In a pilot experiment, we have confirmed that in a CB-treated rat, the frequency and strength of small intestinal contractions are highly reduced in comparison with what is found in a vehicle-treated control rat.
Abalo, R., Vera, G., López-Pérez, A. E., Martínez-Villaluenga, M. & Martín-Fontelles, M. I. I. The gastrointestinal pharmacology of cannabinoids: focus on motility. Pharmacology 90, 1–10 (2012). https://www.ncbi.nlm.nih.gov/pubmed/22699400
Additionally, Cannabis has been shown to reduce stomach acid secretion. Aside from motility, insufficient stomach acid is another factor that increases the risk of SIBO.
In summary, while Cannabis might reduce some IBS symptoms by relaxing the gut, it also makes SIBO relapse more likely by reducing small intestine motility and stomach acid secretion.
